
Diabetic tractional retinal detachments (TRDs) are among the most challenging cases a retina specialist can face. Advances in technology over the last decade have greatly improved outcomes, increased safety, and reduced operating time. These include the evolution of small-gauge vitrectomy from 23-gauge to 27-gauge, the cutter design with the port opening closer to the tip, and an increased cutting rate. In addition to these advances, a wide array of instruments, such as lighted pics and vertical and horizontal scissors available in different gauge sizes, have expanded our armamentarium for treating diabetic TRDs. The introduction of the NGENUITY 3D Visualization System (Alcon) has improved visualization during the fine maneuvers performed in tight spaces over ischemic thin retina, thus minimizing the risk for iatrogenic trauma.
In this article, I present a diabetic TRD repair using the unique advantages of the 25-gauge, high-speed, 10k beveled cutter. The vitrectomy was performed with the CONSTELLATION Vision System (Alcon), and visualization was provided by the NGENUITY 3D system mounted on the OPMI Lumera 700 microscope with the Resight system (Zeiss).
Case Presentation
A 33-year-old patient with type 1 diabetes presented with decreased central vision in his left eye. His VA was 20/100 OD and 20/250 OS. IOPs were 16 mm Hg OU. The anterior segment examination was significant for mild posterior subcapsular cataracts in both eyes. Dilated fundus examination showed proliferative diabetic retinopathy with severe ischemia in both eyes (Figures 1 and 2). The left eye had a macula-involving TRD (Figure 1). Surgery was recommended for the left eye, and the patient received an intravitreal injection of 1.25 mg of bevacizumab (Avastin, Genentech) 1 week prior to the vitrectomy.
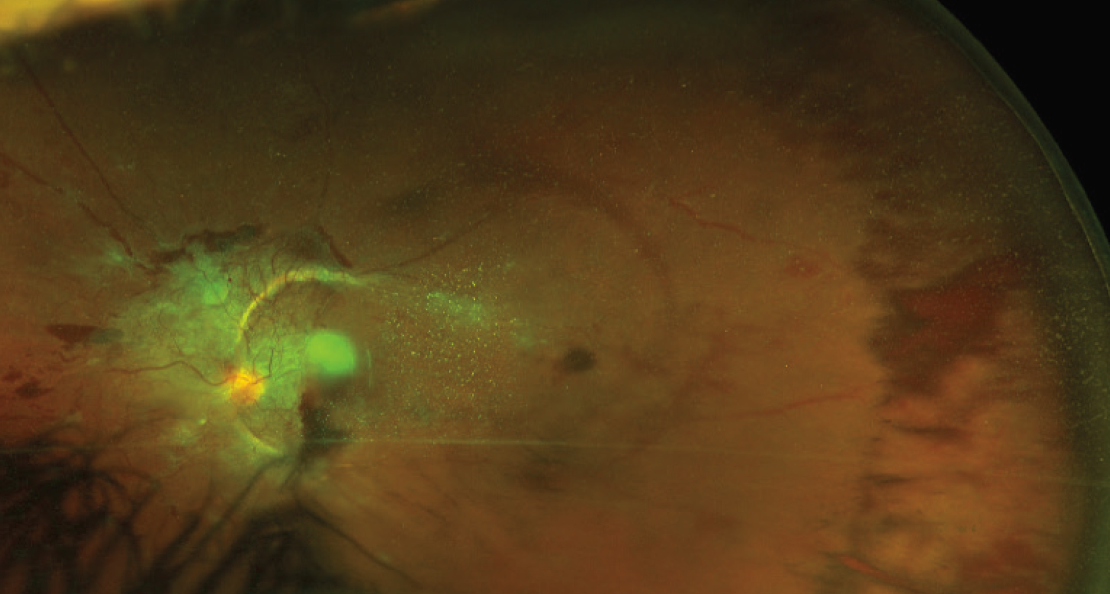
Figure 1. Wide-angle color photograph preoperatively shows vitreous hemorrhage with a TRD involving the macula. Extensive fibrovascular proliferation is present over the optic nerve and along the vascular arcades. VA is 20/250.
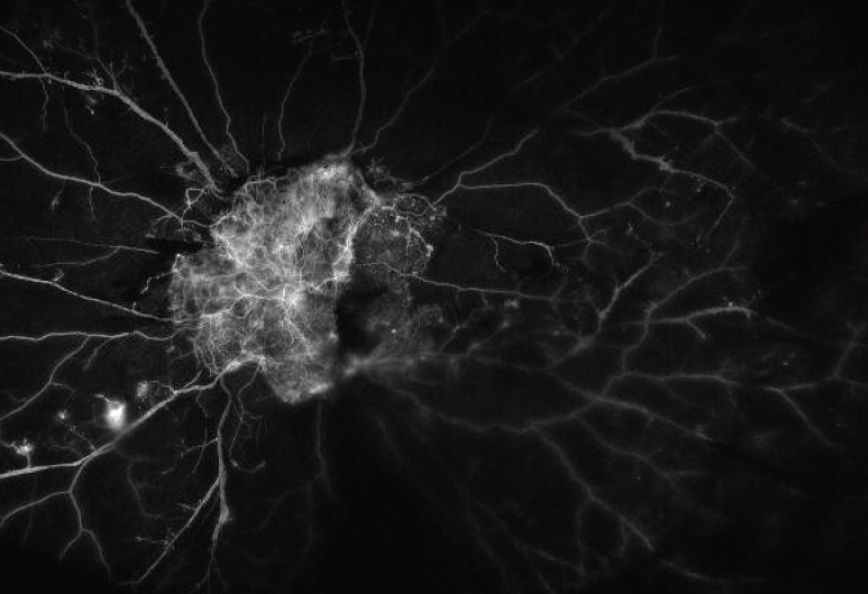
Figure 2. Wide-angle fluorescein angiogram preoperatively shows extensive ischemia 360º; a large neovascular frond over the nerve is visible.
I usually inject bevacizumab preoperatively, as it minimizes bleeding during surgery. It was particularly critical in this case, given the prominent vascularity of the large neovascular frond over the optic nerve and the macula. Timing of the injection before the surgery can be variable, and a recent randomized trial showed that injection 5 to 10 days before the surgery leads to better postoperative outcomes at 6 months and fewer postoperative complications compared to injecting 1 to 3 days before the surgery.1
We proceeded with 25-gauge vitrectomy with the 10k high-speed beveled cutter. After relieving the anterior posterior traction 360º, we focused on the extensive fibrovascular proliferation posteriorly (Figure 3A). The bevacizumab helped significantly, as most of the vessels had regressed, and we could proceed safely to segmentation and delamination of the membranes with minimal bleeding (Figure 3B, C).
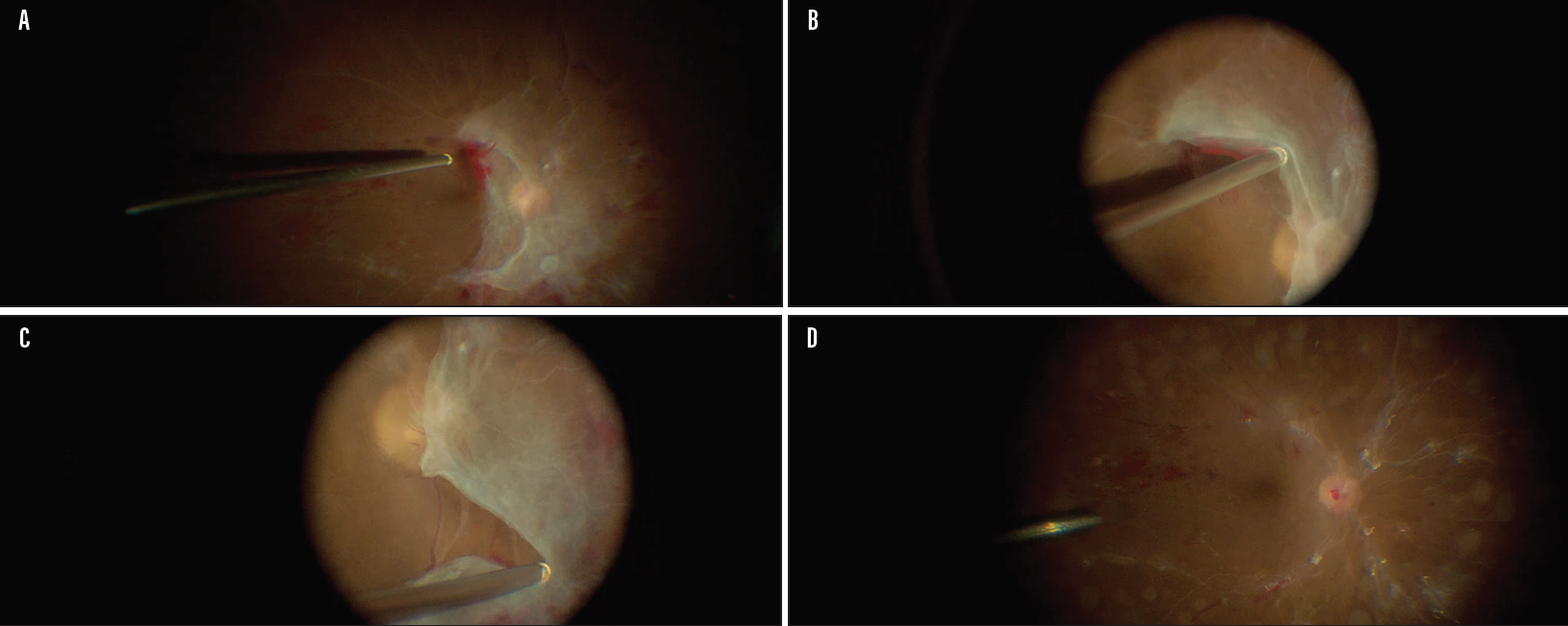
Figure 3. Intraoperative picture shows the extensive fibrovascular membranes posteriorly (A). The cutter is used as a blunt dissector to gently lift the tissue for segmentation (B) as well as for segmentation and delamination of the membranes (C). Intraoperative picture at the conclusion of the surgery showing removal of all tractional membranes without any iatrogenic breaks and LASER spots applied in a PRP fashion (D).
The design of the beveled cutter enabled us to use it as a blunt dissector (Figure 3B, C) as well as vertical scissors. The 25-gauge beveled cutter provides 50% closer proximity to the retina when held at a tangential angle at 60º compared to the flat-tip cutter. In addition, the distance between the tip of the cutter to the port opening is 0.009 inches in the beveled 25-gauge tip compared to 0.017 inches in the regular tip, which represents a 47% decrease.
Furthermore, the high cutting speed (10k) minimized movement of the detached retina, allowing for safe and efficient removal of all fibrovascular membranes and the posterior hyaloid. These features allowed us to segment and delaminate every membrane without using a second instrument and without any breaks.
After all membranes were removed, triamcinolone was injected in the vitreous cavity, and more vitrectomy was performed to clean up any residual vitreous posteriorly as well as in the periphery under scleral depression. Light amplification by stimulated emission of radiation (LASER) was applied in a panretinal photocoagulation fashion 360º to the ora serrata with the curved endolaser lighted probe (Figure 3D). Fluid-air exchange was performed, and the air was exchanged with a dilute mixture of 18% SF6 (Video).
Thanos Papakostas, MD, describes a diabetic tractional retinal detachment (TRD) repair on a 33-year-old male with severe proliferative diabetic retinopathy (PDR) and ischemia using the 25-gauge high-speed beveled cutter from Alcon.
Two months after surgery, the patient’s VA has improved to 20/40 with attached retina (Figure 4).
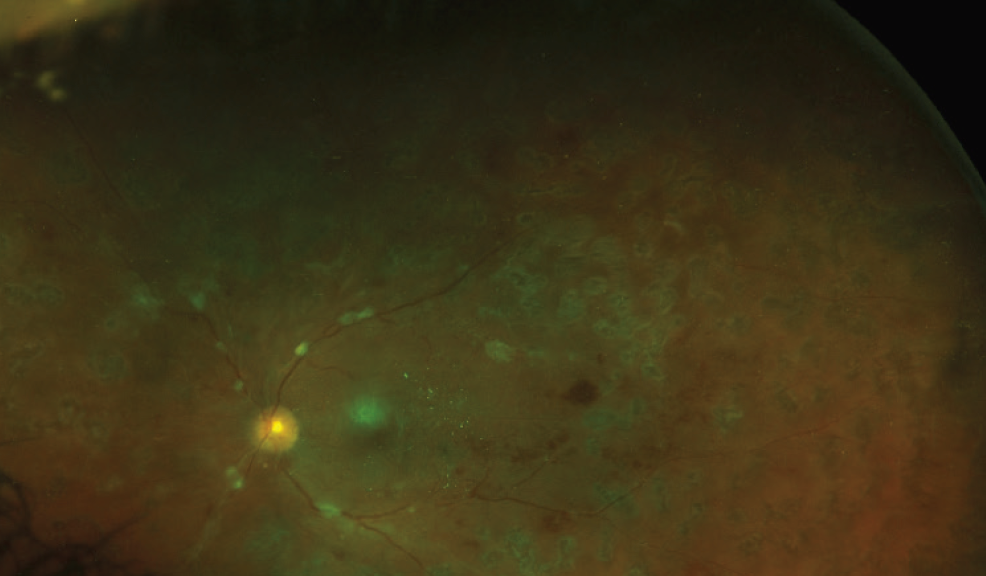
Figure 4. Wide-angle color photograph postoperatively. Two months after surgery, the retina is attached, and the VA has improved to 20/40.
Discussion/conclusion
The most important step of a diabetic TRD repair is the removal of the posterior hyaloid and all fibrovascular membranes exerting traction on the retina, either with an inside-out fashion, starting from the optic nerve and moving out, or an outside-inside fashion, starting from the edge of the membanes and moving toward the optic nerve, as we did in this case.
This case highlights the versatility of the 25-gauge, high-speed beveled cutter in the repair of a complex diabetic TRD. Its design enables the surgeon to use it as a pic, blunt dissector, forceps, and vertical scissors. Usually, a second instrument, such as a lighted pic, or a bimanual approach with forceps and scissors under chandelier illumination is commonly employed in these complicated retinal detachments. In this case, however, we were able to safely and efficiently segment and delaminate all membranes with the cutter only. Also, the absence of a rhegmatogenous component in this case made cutter delamination feasible, as there was enough inherent countertraction that opposed the forces exerted by the cutter delamination and dissection maneuvers.2
The techniques used to perform cutter delamination are foldback delamination and conformal cutter delamination, as previously described by Charles.3 Foldback delamination can be achieved when the surgeon places the cutter on the anterior edge of the epiretinal membrane just behind the leading edge. Conformal cutter delamination happens when the cutter is constantly rotated along the long axis to cause rotation of the port away from the retina while maintaining apposition of the cutter port to the fibrovascular membrane. Another key element of this case was that the NGENUITY 3D Visualization System provided a high degree of stereopsis during the fine maneuvers on the posterior pole. This, in addition to the lower illumination levels used, increased safety during surgical maneuvers. Implementation of the latest technological advancements in instrumentation and visualization in vitreoretinal surgery can help us safely and efficiently repair complex retinal detachments, such as diabetic TRD.
1. Castillo J, Aleman I, Rush SW, Rush RB. Preoperative bevacizumab administration in proliferative diabetic retinopathy patients undergoing vitrectomy: a randomized and controlled trial comparing interval variation. Am J Ophthalmol. 2017;183:1-10.
2. Adam M. Gauging diabetic TRDs. New Retina MD. December 2017. http://nrmdonline.com/2017/12/gauging-diabetic-trds. Accessed July 27, 2018.
3. Charles S. Curved scissors delamination. Retina Today. Jan/Feb 2012. http://retinatoday.com/2012/02/curved-scissors-delamination. Accessed July 23, 2018.

