
Case Background
- A case of a 67-year-old white man with an 11-year history of diabetes mellitus.
- The hemoglobin A1C was 8.6, and the patient had hypertension, a past history of myocardial infarction, and he was an active smoker.
- Medications included metoprolol, aspirin, and metformin.
- Past ocular history included cataract extraction and placement of a posterior chamber IOL in each eye.
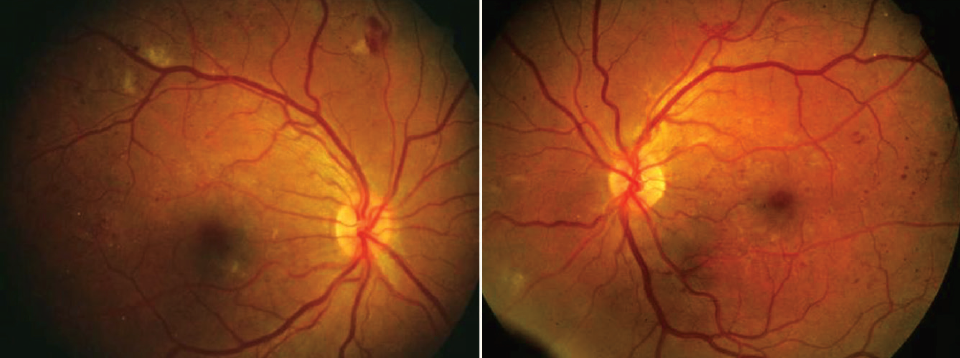
Figure 1. Fundus photographs show moderately severe to severe nonproliferative DR at baseline.
Initial Treatment Plan
- Fundus photography showed moderately severe to severe nonproliferative diabetic retinopathy (DR) in both eyes, and VA was 20/25 OU (Figure 1).
- I showed images to the patient and explained how diabetes damages blood vessels, noted that the blood is leaking out, and said those little white spots are little mini infarcts, like little mini heart attacks in the retina.
- I mentioned the possibility of reversing the disease course with anti-VEGF agents, but he was resistant to starting treatment.
- We concluded the visit without starting treatment and scheduled a recheck in 3 months, and I was hopeful of continuing the conversation at that point.
Missed Follow-Up and Recovery Plan
- The patient did not return until 15 months later with more severe retinopathy in each eye, but it was significantly worse in the right eye (Figure 2).
- An anti-VEGF injection was given in the right eye, followed by vitrectomy 1 week later with membrane peeling, endolaser, and silicone oil.
- In the left eye, monthly anti-VEGF injections were continued to regress the now proliferative DR, and ultimately, panretinal photocoagulation was performed due to risk of being lost to follow-up.
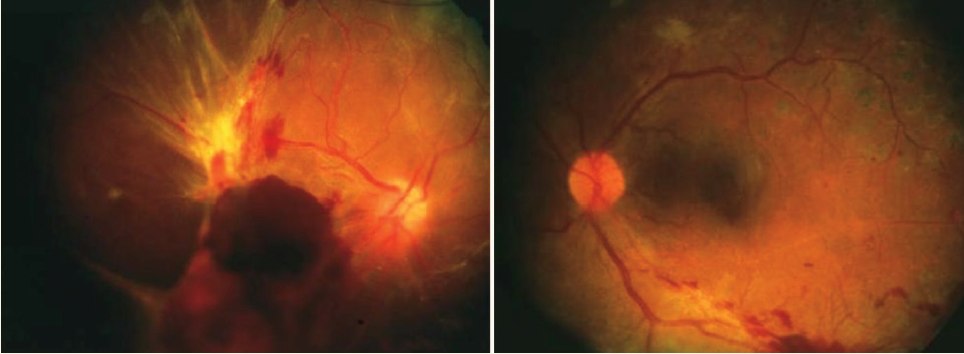
Figure 2. After being lost to follow-up for 15 months, the same patient as in Figure 1 returned with extensive worsening of the DR.
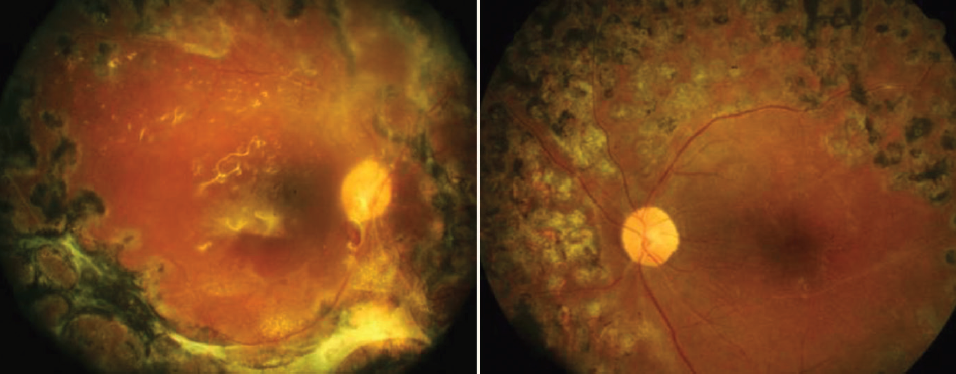
Figure 3. Fundus photographs 2 years after the initial presentation showing marked deterioration of the status of the retina.
Conclusion
This was an unfortunate case where the status of the retina deteriorated over time, and VA was eventually counting fingers in the right eye and 20/50 in the left (Figure 3). I would call this a treatment failure because it was a failure to properly communicate the severity of DR to the patient and to encourage compliance with the recommended treatment. This is likely a situation that is familiar to many practicing retina specialists. While the majority of our patients are engaged in their care, this case highlights that patients simply do not comprehend their disease or appreciate the consequences of ignoring their doctor’s recommendations for treatment. We should not be seeing cases of DR that wind up like this in 2018, because we have ways to prevent worsening DR and vision loss. To me, that is really what the anti-VEGF era for DR is all about.
