Patient History
- 77-year-old woman with distortion in her left eye, 3 weeks in duration; right was asymptomatic and showed dry AMD
- VA was 20/25 OD, 20/60 OS
- OCT showed central subretinal fluid (SRF) with Type 1 choroidal neovascularization, which was confirmed with a fluorescein angiogram that also showed ill-defined central leakage (Figure 1)

Figure 1. OCT and fluorescein angiogram at the initial visit before treatment.
Intervention
- Anti-VEF therapy with aflibercept (Eylea, Regeneron) was started OS
- Two monthly injections resulted in resolution of SRF and VA improved to 20/30 (Figure 2)
- The interval was extended, first to 6 weeks, followed by 8 weeks, at which time SRF returned (Figure 3)

Figure 2. Two injections given at 1-month intervals led to resolution of SRF and improved vision.
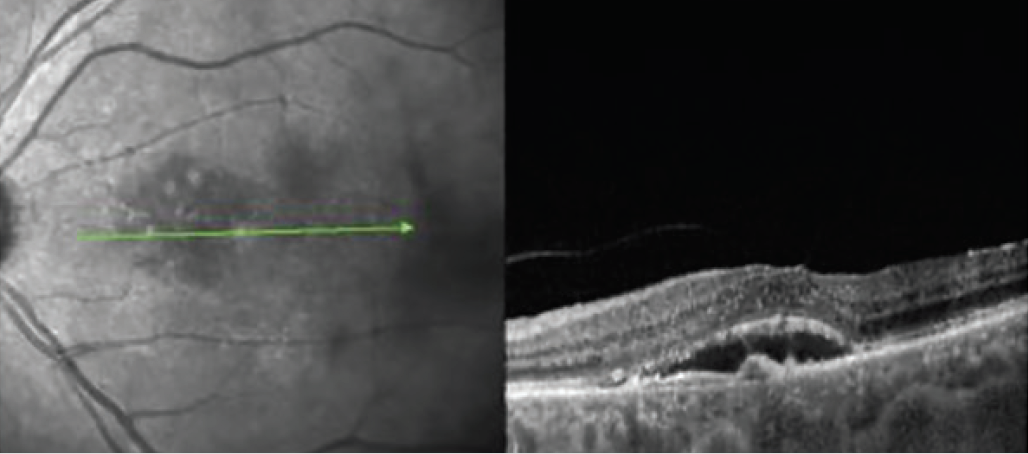
Figure 3. Extension to 6 week intervals was successful at maintaining anatomic control, but shifting to an 8-week retreatment interval resulted in reaccumulation of SRF.
Discussion
Carl D. Regillo, MD: There’s a lot of talk in the literature and on the podium about whether we can tolerate certain degrees of recurrent fluid or SRF. Is this something you are going to tolerate or something you are going to act on in terms of changing the management?
Rishi P. Singh, MD: I’m slightly confused by what the fluid argument should be now. We just did an analysis on our own patients in routine clinical practice. We found that SRF was protective and intraretinal fluid was negative prognosticator of outcomes at both 12 months and 24 months.
Dr. Regillo: I felt compelled to reduce the interval to try to get back to optimal exudative control. Would anyone do anything different?
Caroline R. Baumal, MD: Fluid is a biomarker. When we’re doing clinical studies, looking at fluid on OCT, we’re not always getting the tempo of the fluid. But that’s something we can get when we see our patients. The level of the activity, the change of the vision, and what we know from clinical studies that the more injections patients get, the better their visual outcomes are over time, would lead me to inject this patient and go back to 4-week intervals.
Usha Chakravarthy, MD, PhD, CBE: I can’t see that, in this early phase of the patient’s treatment trajectory that this should tolerated. Five years down the line, if I saw this, I might be more inclined to tolerate it. The question is whether you’d go back to 6 weeks or 4 weeks. My personal preference would be reduce back to 6 weeks to see how well this patient has returned to her 6 week baseline.
Dr. Regillo: That’s exactly what we did. And that’s typically what I do, unless it’s a major setback. I go back to the last exudative-free interval, which was 6 weeks (Figure 4). VA returned to 20/30. From this point, there are a lot of questions we could ask: Does that interval become fixed now for this patient? Do we consider switching drugs? My personal view is, when in practice, I usually keep patients at least a few cycles at this interval, let the condition settle down, and then maybe re-challenge 6 months later to see if that interval is going to change over time.

Figure 4. The interval was shortened to 6 weeks, which provided greater control.
Dr. Singh: We don’t really know the interval until you go later in stages. I don’t think it’s unreasonable to rechallenge the patient to potentially go 8 weeks again, or even 10 weeks again, if their fluid resolves.